The Complete Expert Guide to Advanced Non-Surgical Back Pain Care at IBAP Clinics, Hyderabad
Written & Reviewed by Dr. Vijay Bhaskar Bandikatla | IBAP Clinics, Hyderabad | April 2026
TL;DR — What You Need to Know
Chronic back pain does NOT always require surgery. Research shows 10–40% of spine operations result in persistent pain, and 85% of MRI findings are also present in pain-free people. At IBAP Clinics, Hyderabad, Dr. Vijay Bhaskar Bandikatla (FRCA, FFPMRCA, CCT UK — trained at Cambridge and London) offers the most advanced non-surgical treatment portfolio in India: precision intradiscal procedures, joint ablations, vertebral augmentation for osteoporotic fractures, epiduroscopy for post-surgical scarring, and neuromodulation for intractable pain — all performed under live fluoroscopic or ultrasound guidance, the same precision imaging used in cardiac angiography.
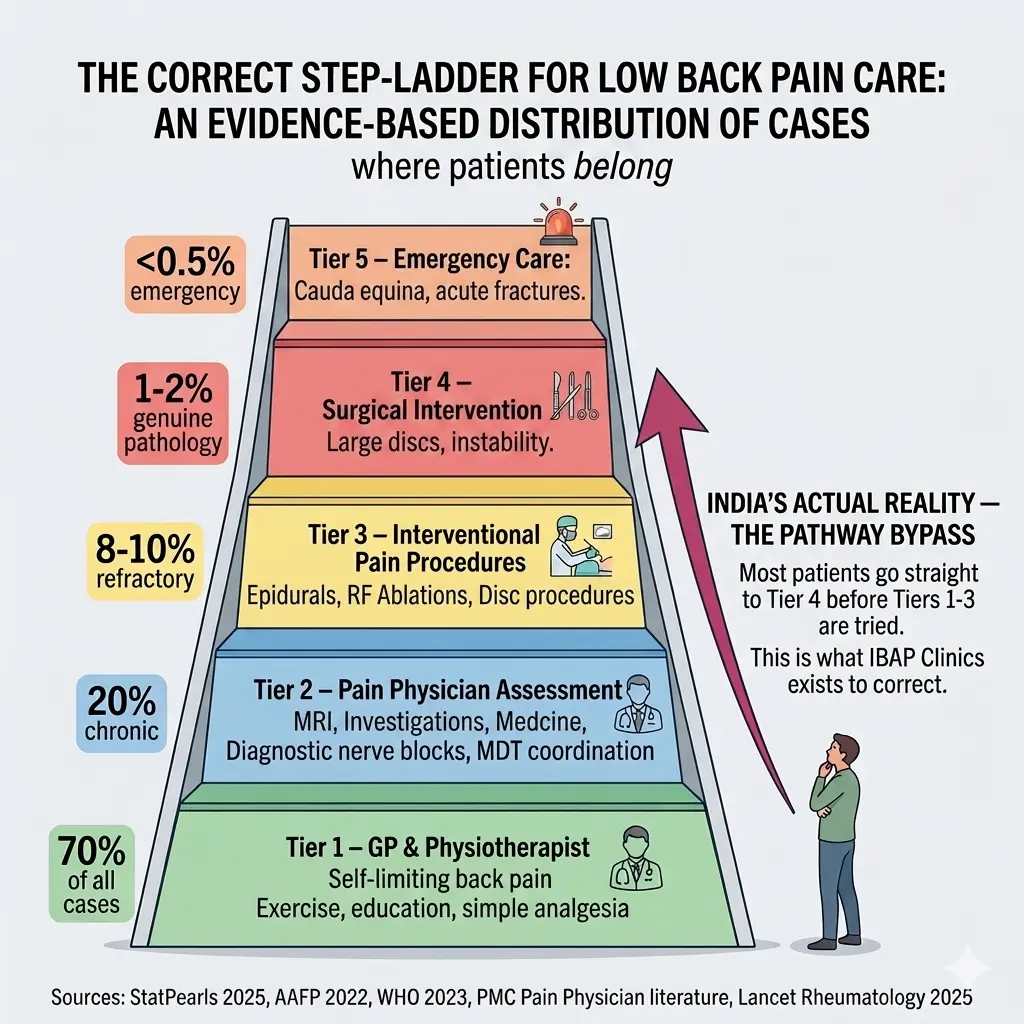
India's Upside-Down Back Pain Pyramid — Why the Current System is Failing Patients
In Western healthcare systems — the UK, Australia, the United States — back pain management follows a clear evidence-based pyramid. At the broad base sits the General Physician (GP) and community physiotherapist, managing 80–90% of cases conservatively. At the narrow tip sits the surgeon, who intervenes only when all other pathways have been genuinely exhausted.
In India, this pyramid is frequently inverted. A patient with a week-old backache often walks directly into a Neurosurgeon’s or Orthopaedic Surgeon’s consulting room. Once there, the conversation naturally gravitates towards MRI scans and operative options — bypassing the critical middle layers of care that could resolve the problem without a single incision.
The Numbers Don't Lie — Why This Matters
- 10–40% of spine surgeries result in Failed Back Surgery Syndrome (FBSS) — persistent pain despite technically successful operations.
-
Patient satisfaction after spinal fusion drops from 80% in year one to just 22% after several years as Adjacent Segment Disease develops.
-
85% of imaging findings (disc bulges, wear and tear) are also present in people with absolutely no pain — meaning the MRI may be finding a coincidental finding, not your pain source.
-
Hardware complications including screw loosening (~22.5% incidence) and biocorrosion occur even with perfect surgical technique.
- Guideline adherence for conservative care in India remains at only 23–34% — the system is structured to operate before it rehabilitates.
At IBAP Clinics, Dr. Vijay Bhaskar Bandikatla is committed to restoring the pyramid to its correct orientation — ensuring every patient gets the right treatment, from the right specialist, at the right time. That begins with an accurate diagnosis and an honest, unbiased second opinion.
The Second Opinion Advantage — Before You 'Go Under the Knife'
Why MRIs Can Be Misleading — 'Treating the Image, Not the Patient'
A landmark systematic review (Brinjikji et al., American Journal of Neuroradiology, 2015) found that disc bulges, degeneration, and ‘wear and tear’ are present on MRI in a large majority of completely pain-free adults. The real pain generator is often an inflamed facet joint, a torn disc annulus, a sacroiliac joint dysfunction, or a sensitised nerve — none of which show clearly on routine MRI. At IBAP Clinics, diagnostic precision nerve blocks act as a functional ‘GPS for the spine’ — confirming the true pain source before any permanent changes are made.
What Our Second Opinion Consultation Covers
- Full review of your diagnosis, scans, and previous treatment history
- Honest explanation of the true risks and realistic benefits of the proposed surgery
- Functional diagnostic assessment — identifying your actual pain generator, not just the MRI finding
- Presentation of all available non-surgical, minimally invasive, and staged alternatives
- Identification of whether you are a high-risk candidate for hardware failure (osteoporosis, lifestyle factors)
- The final decision is always yours — made with complete, unbiased information, never under pressure
When Surgery IS Genuinely Necessary
Surgery remains essential for specific urgent conditions — and at IBAP Clinics, we will tell you honestly when you need it. Clear surgical indications include: progressive nerve compression with objective muscle weakness or wasting; spinal instability (spondylolisthesis grade III–IV); cauda equina syndrome with loss of bowel or bladder control; spinal tumour or infection; and acute vertebral fractures with neurological compromise. Everything else warrants a prior specialist pain physicians opinion.
The Technology That Makes It Possible — Fluoroscopy & Ultrasound Guidance
The Cardiac Angiography Analogy
A cardiologist would never stent a blocked coronary artery without real-time X-ray guidance — the consequences of imprecision are unacceptable. Exactly the same principle applies pain patients at IBAP Clinics. We treat your spine with the same imaging standard used in cardiac catheterisation laboratories. The needle goes precisely where it needs to go — millimetre by millimetre, confirmed on live imaging — not approximately. The result: smaller needles, higher accuracy, fewer complications, and faster recovery. Most procedures are completed in 20–45 minutes as a day case, with patients returning home the same afternoon.
Nerve & Radicular Pain: Epidural Injections & Nerve Blocks
Epidural Steroid Injections (ESI)
Anti-inflammatory corticosteroid is delivered under fluoroscopic guidance directly into the epidural space surrounding the irritated nerve root. This washes out the inflammatory mediators driving nerve swelling and pain — providing meaningful relief lasting weeks to months. This relief creates a vital rehabilitation window. Caudal epidural steroid injections carry Level I evidence from the American Society of Interventional Pain Physicians (ASIPP) for short-term radicular pain relief.
Analogy : Dousing a fire at its precise source rather than spraying water at the smoke — the ESI delivers the anti-inflammatory agent exactly where the nerve is on fire, not broadly into the bloodstream.
Targeted Diagnostic & Therapeutic Nerve Blocks
Selective nerve root blocks serve a critical dual purpose: confirming which specific nerve or joint is generating your pain (diagnostic), then providing immediate therapeutic relief. Under fluoroscopic guidance, a fine needle is steered to the exact nerve root — acting as a precise GPS for your spine, eliminating diagnostic guesswork. This diagnostic clarity is what separates specialist pain medicine from generic treatment. These procedures can in turn guide the spinal surgeon for targetted surgical procedures when necessary.
Analogy : Turning off individual circuit breakers in a fuse box one at a time — rather than cutting power to the entire building, we identify exactly which circuit is faulty before deciding how to fix it.
Advanced Intradiscal Procedures: Treating the Disc from Within
Ozone Disc Nucleolysis (Oxygen-Ozone Therapy)
A precisely calibrated medical-grade oxygen-ozone mixture is injected into the herniated disc under fluoroscopic guidance. Ozone fragments the glycosaminoglycans (water-retaining molecules) within the disc nucleus — reducing its volume and intradiscal pressure, drawing the herniation away from the compressed nerve. Simultaneously, ozone modulates the immune environment, switching the disc from an inflammatory to a reparative state and promoting myelin sheath regeneration around damaged nerves. A retrospective analysis of 2,089 patients (Pain Physician) reported VAS pain scores falling from 7.73 to 1.36 at one year — an 80%+ sustained reduction. A 2025 prospective study (Kharrat et al.) confirmed pain improvement in 85% of patients. Results are comparable to surgery in patients without neurological deficit.
Analogy : An over-inflated tyre pressing against the rim — ozone is the controlled release valve, reducing internal disc pressure so the bulge retracts away from the nerve root.
Disc Biacuplasty (Cooled Radiofrequency for Discogenic Pain)
For chronic ‘deep’ back pain arising from inside a degenerated disc — where pain-conducting nerve fibres have grown into annular tears and fissures — Biacuplasty targets them with precision. Two cooled radiofrequency probes are inserted bilaterally into the disc under fluoroscopic guidance, delivering controlled thermal energy to deactivate pain-transmitting nerve fibres within the disc wall, while simultaneously consolidating and strengthening the annular structure. The cooled technology creates a larger, safer lesion than conventional intradiscal techniques. Unlike disc removal, the disc’s structural integrity is preserved.
Analogy: Two precisely placed heating elements inside a cracked pipe — gently sealing the cracks from within rather than replacing the entire pipe.
Laser Disc Decompression (PLDD — Percutaneous Laser Disc Decompression)
A fine laser fibre is introduced through a needle into the disc nucleus under fluoroscopic guidance. A controlled burst of laser energy vaporises a small volume of nucleus pulposus — creating a vacuum effect that draws the herniated disc material away from the trapped nerve root. Because the nucleus is a closed hydraulic system, a small reduction in volume produces a disproportionately large reduction in intradiscal pressure. Completed in under 30 minutes with no surgical incision and a rapid return to activity.
Analogy: Squeezing a small amount of toothpaste from the middle of a tube — even a small reduction in the core creates enough room for the rest to redistribute, relieving pressure on the nerve.
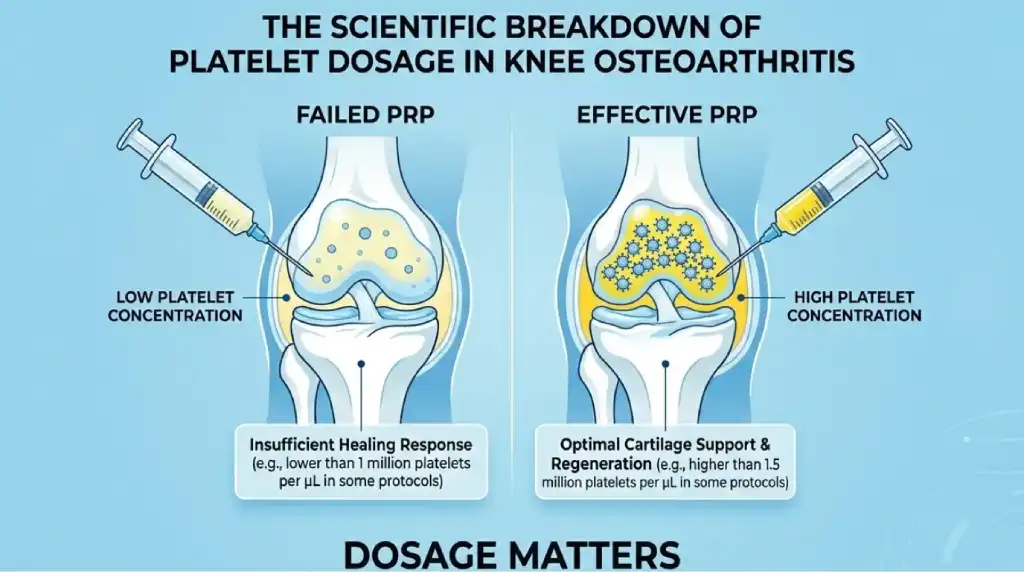
Regenerative Intradiscal Therapy — PRP & BMAC
Platelet-Rich Plasma (PRP) or Bone Marrow Aspirate Concentrate (BMAC) — prepared from the patient’s own blood or bone marrow — are injected directly into degenerated discs, facet joints, or the sacroiliac joint. These preparations contain concentrated growth factors that promote disc matrix repair, reduce inflammation, and support tissue regeneration. Because patient-derived biological material is used, the risk of adverse reactions is exceptionally low. A 2025 ASIPP evidence update confirmed fair supporting evidence for PRP in discogenic and facet applications.
Analogy: Sending your spine’s own repair crew directly to the site of damage — concentrated healing factors your body already makes, delivered precisely where they are most needed.
Facet & Sacroiliac Joint Pain: Precision Joint Ablations
Radiofrequency Ablation (RFA) — Medial Branch & Sacroiliac Joint
Following diagnostic confirmation with medial branch nerve blocks, RFA uses fluoroscopy-guided controlled radiofrequency energy to thermally interrupt the specific nerves carrying pain from arthritic facet or sacroiliac joints — providing 6–18 months of relief per treatment. The 2025 RAPID study (Interventional Pain Medicine, Provenzano et al.) confirmed sustained clinically meaningful reductions in both NRS pain scores and ODI disability scores in real-world patients. The procedure is safely repeatable, with each subsequent treatment providing a further 10–16 months of benefit in responders.
Analogy: A persistent fire alarm that cannot be silenced — RFA severs the wire between the alarm (arthritic joint) and the control panel (your brain), providing lasting quiet without demolishing the building.
Pulsed Radiofrequency (PRF) to the Dorsal Root Ganglion (DRG)
For radicular (nerve root) pain where thermal ablation is not appropriate, PRF delivers short bursts of radiofrequency energy to the Dorsal Root Ganglion — the pain relay station — modulating pain transmission without creating a destructive lesion. A landmark 2025 double-blind RCT (Zeng et al., Regional Anaesthesia & Pain Medicine) confirmed 6 minutes of PRF to the DRG delivers the optimal balance of efficacy and durability for lumbar radiculopathy.
Analogy: A noise-cancelling signal sent to a radio receiver — PRF scrambles the incoming pain signal before it reaches the brain’s perception centres, without destroying the receiver itself.
Osteoporotic Vertebral Fractures: Vertebroplasty & Kyphoplasty
Vertebroplasty — Immediate Fracture Stabilisation
Under fluoroscopic guidance, medical-grade bone cement (PMMA) is injected through a fine needle directly into the collapsed vertebral body. The cement sets within minutes — restoring structural integrity, dramatically reducing pain, and enabling the patient to mobilise the same day. Evidence from multiple systematic reviews confirms rapid, significant pain reduction and functional improvement in acute osteoporotic VCFs. The procedure prevents progressive collapse and the downstream complications that follow untreated fractures.
Analogy: Filling a pothole in a road before it caves in — injecting structural material to restore load-bearing capacity and prevent the surface from collapsing further.
Kyphoplasty — Stabilisation with Height & Posture Restoration
Kyphoplasty advances on vertebroplasty by first inflating a small balloon inside the collapsed vertebral body under fluoroscopic guidance — partially restoring the lost height and creating a defined cavity for cement. This two-stage process not only stabilises the fracture but also corrects spinal deformity (kyphosis), improving posture and reducing respiratory and neurological risks from progressive collapse. Particularly valuable for subacute fractures where height restoration remains possible. Both procedures are performed as day cases under local anaesthesia and sedation.
Analogy: Inflating a balloon inside a crushed tin can before filling it with concrete — the balloon reshapes the structure first, then the cement locks it in its corrected form permanently.
Failed Back Surgery Syndrome: Epidural Adhesiolysis, Epiduroplasty & Epiduroscopy
Epidural Adhesiolysis — The Racz Neuroplasty Procedure
Developed by Dr. Gabor Racz in the late 1980s, this technique involves passing a steerable catheter through the sacral hiatus (caudal approach) into the epidural space under fluoroscopic guidance. Contrast imaging delineates the extent of scarring and identifies which nerve roots are tethered. The catheter is then steered to mechanically disrupt the adhesions, freeing the compressed nerve. Hyaluronidase, local anaesthetic, and corticosteroid are delivered precisely to the freed nerve — reducing inflammation and inhibiting re-adhesion. Systematic reviews confirm clinically relevant reductions in pain and disability scores at 6–12 months in FBSS patients. Performed as a day case at IBAP Clinics.
Analogy: A skilled locksmith working inside a seized lock — carefully freeing the mechanism without breaking down the entire door.
Epiduroscopy — Direct-Vision Adhesiolysis
Epiduroscopy is the most advanced approach to FBSS treatment. A fibre-optic spinal endoscope — a miniature live camera on a flexible catheter — is introduced into the epidural canal. This provides direct visualisation of scar tissue, inflamed nerve roots, and adhesions in real time, enabling far more targeted and complete adhesiolysis than blind catheter-based techniques. Medications are delivered with pinpoint accuracy directly to the affected nerve root. A systematic review and meta-analysis (Geudeke et al., Pain Practice, 2021) confirmed VAS scores falling from 7.6 at baseline to 4.3 at 12 months — a clinically meaningful sustained reduction. Studies show significantly greater long-term benefit in patients with nerve root adhesions.
Analogy: Keyhole surgery with a live camera — rather than working blind, the specialist sees exactly where scar tissue has tethered nerve roots, cuts it under direct vision, and confirms the nerve is free before withdrawing.
Intractable & Refractory Pain: Neuromodulation
Spinal Cord Stimulation (SCS) — The Pain Pacemaker
Thin electrical leads are placed in the epidural space adjacent to the spinal cord under fluoroscopic guidance and connected to a small, programmable pulse generator — a ‘pain pacemaker’ — implanted beneath the skin. This delivers mild, adjustable electrical impulses that intercept pain signals before they reach the brain’s perception centres. Every patient undergoes a 7–10 day external trial with a temporary device before any permanent implant decision. A 2024 meta-analysis confirmed high-frequency SCS provides durable long-term pain relief and functional improvement. A 2024 retrospective series combining DRG + SCS achieved an average 79% pain reduction in 94% of patients. Modern devices are fully MRI-compatible, rechargeable, and programmable via smartphone, with battery life exceeding 10 years.
Analogy: Noise-cancelling headphones for the spinal cord — the device generates a counter-signal that drowns out the pain signal before it reaches the brain. You feel a gentle background sensation instead of debilitating pain.
Intrathecal Drug Delivery Systems (IDDS) — The Pain Pump
A small titanium pump implanted beneath the abdominal skin wall delivers medication via a fine catheter directly into the intrathecal space — the cerebrospinal fluid surrounding the spinal cord. Because the drug acts directly at spinal cord level, doses as small as 1/300th of the equivalent oral dose achieve superior pain control with dramatically fewer systemic side effects (sedation, nausea, constipation). The pump is refilled every 3–6 months via a simple outpatient injection. Particularly effective for intractable cancer pain, severe spasticity, and complex chronic pain refractory to all other measures.
🔍 Analogy: Precision drip irrigation versus a watering can — oral medication is absorbed throughout the entire body, whilst an intrathecal pump delivers medication directly to the root of the problem. Maximum effect. Minimum dose. Minimum side effects.
Complete Treatment Portfolio — IBAP Clinics at a Glance
| Procedure | Best For | Relief Duration | Image Guidance |
|---|---|---|---|
| Epidural Steroid Injection | Disc herniation, sciatica, spinal stenosis | Weeks–months | Fluoroscopy |
| Diagnostic Nerve Block | Nerve root pain — diagnostic & therapeutic | Diagnostic | Fluoroscopy / Ultrasound |
| Radiofrequency Ablation (RFA) | Facet & sacroiliac joint pain | 6–18 months | Fluoroscopy / Ultrasound |
| Pulsed RF / DRG Stimulation | Radicular / nerve root pain | 6–12 months | Fluoroscopy / Ultrasound |
| Ozone Disc Nucleolysis | Disc herniation, nerve compression | Long-term (1+ yr) | Fluoroscopy / Ultrasound |
| Disc Biacuplasty | Chronic internal disc pain | Long-term | Fluoroscopy |
| Laser Disc Decompression (PLDD) | Contained disc herniation | Long-term | Fluoroscopy |
| PRP / BMAC Regenerative | Disc, facet & sacroiliac degeneration | Variable | Fluoroscopy / Ultrasound |
| Vertebroplasty | Osteoporotic vertebral fracture | Immediate & lasting | Fluoroscopy |
| Kyphoplasty | VCF + vertebral height restoration | Immediate & lasting | Fluoroscopy |
| Epidural Adhesiolysis | Failed back surgery syndrome | 6–12+ months | Fluoroscopy |
| Epiduroscopy | Camera-guided adhesiolysis | 6–12+ months | Fluoro + Camera |
| Spinal Cord Stimulation (SCS) | Chronic post-surgical pain | Long-term (10+ yr) | Fluoroscopy |
| Intrathecal Drug Pump | Intractable & cancer pain | Long-term | Fluoroscopy |
| Second Opinion Consultation | Pre-surgical review | N/A | Clinical + Imaging |
Why Trust IBAP Clinics?
About the Author & Reviewer — Dr. Vijay Bhaskar Bandikatla
Dr. Vijay Bhaskar Bandikatla is an Interventional Pain Specialist and Founder of Indo British Advanced Pain Clinics (IBAP Clinics), Hyderabad. He holds MBBS, DA, FRCA (Fellow of the Royal College of Anaesthetists, London), FFPMRCA (Fellow of the Faculty of Pain Medicine, London), CCT (UK) in Pain Medicine, Advanced Pain Training (Cambridge), DDSMed (Diploma in Sports Medicine, Chicago), and a Fellowship in Neuromodulation and Advanced Pain (London). He returned to India to establish specialist pain services of British standard and serves as Senior Consultant at Apollo Hospitals, Hyderabad,. He is also a partner in the Malla Reddy Vishwavidyapeeth Pain Fellowship programme — training India’s next generation of interventional pain specialists. Every clinical article and recommendation at IBAP Clinics is authored and reviewed by Dr. Bandikatla, reflecting direct specialist experience and current international peer-reviewed evidence.
Credentials & Qualifications
- MBBS, DA — Foundation training
- FRCA — Royal College of Anaesthetists, London
- FFPMRCA — Faculty of Pain Medicine, London
- CCT (UK) in Pain Medicine
- Advanced Pain Training — University of Cambridge
- Fellowship in Neuromodulation & Advanced Pain — London
- DDSMed (Sports Medicine) — Chicago
- MBA (Hospital Management)
Clinical Positions & Affiliations
- Senior Consultant — Apollo Hospitals, Hyderabad
- Founder & Director — IBAP Clinics, Banjara Hills
- Founder & Director — IBAP Clinics, Madeenaguda
- Partner — Malla Reddy Vishwavidyapeeth Pain Fellowship
- Member — Indian Society for Study of Pain (ISSP)
Frequently Asked Questions:
Yes — and it should be the first approach. At IBAP Clinics, Hyderabad, Dr. Vijay Bhaskar Bandikatla (FRCA, FFPMRCA, CCT UK) offers the most comprehensive non-surgical portfolio in India: epidurals, nerve blocks, ozone disc nucleolysis, disc biacuplasty, laser disc decompression, radiofrequency ablation, vertebroplasty, kyphoplasty, epidural adhesiolysis, epiduroscopy, spinal cord stimulation, and intrathecal drug delivery. All procedures are performed under live fluoroscopic or ultrasound guidance. Studies show that 10–40% of spine surgeries result in Failed Back Surgery Syndrome — making a specialist pain opinion before surgery essential.
Yes. Ozone disc nucleolysis is a needle-only, fluoroscopy-guided procedure that reduces disc volume, intradiscal pressure, and local inflammation simultaneously. A retrospective study of 2,089 patients reported VAS pain scores falling from 7.73 at baseline to 1.36 at one year — a sustained 80%+ reduction. A 2025 prospective study (Kharrat et al.) confirmed pain improvement in 85% of patients. Results are comparable to surgery in patients without neurological deficit, making it the preferred pre-surgical alternative for contained disc herniations.
Always — before any elective spinal fusion or discectomy. Research shows that 85% of imaging findings (disc bulges, wear and tear on MRI) are also present in people with zero pain. The real pain generator is often a facet joint, inflamed nerve root, or ligamentous issue that an MRI cannot detect. 10–40% of spine surgeries result in Failed Back Surgery Syndrome. Adjacent Segment Disease means fused vertebrae increase stress on adjacent levels — potentially creating new problems. Patient satisfaction after spinal fusion plummets from 80% in year one to just 22% after several years. A specialist pain physician at IBAP Clinics can diagnose your true pain source and offer targeted, reversible alternatives before any permanent surgical changes are made.
Failed Back Surgery Syndrome (FBSS) is primarily caused by post-surgical epidural fibrosis — scar tissue that forms around nerve roots. Revisional surgery is effective in only 5–30% of cases. At IBAP Clinics, Dr. Bandikatla offers epidural adhesiolysis (the Racz neuroplasty procedure), epiduroplasty, and epiduroscopy — minimally invasive procedures that break down scar tissue using a steerable device under fluoroscopic or direct camera guidance and deliver targeted anti-inflammatory treatment to freed nerve roots. For severe or refractory FBSS, spinal cord stimulation has the strongest long-term evidence of any treatment modality.
Both procedures treat osteoporotic vertebral compression fractures — when weakened bone collapses due to osteoporosis, sometimes from something as minor as a cough. Vertebroplasty injects medical-grade bone cement under fluoroscopic guidance to stabilise the fracture immediately, allowing the patient to mobilise the same day. Kyphoplasty first inflates a small balloon to restore vertebral height before cementing — correcting spinal deformity (kyphosis) and reducing respiratory risks from progressive collapse. Both are day-case procedures with pain relief within 24–48 hours and no major surgery.
Spinal cord stimulation (SCS) — the 'Pain Pacemaker' — places programmable electrical leads in the epidural space to intercept pain signals before they reach the brain. A 7–10 day external trial is always conducted before permanent implantation. Indicated for failed back surgery syndrome, complex regional pain syndrome, severe neuropathic back and leg pain, and refractory chronic pain. A 2024 meta-analysis confirmed high-frequency SCS provides durable long-term pain relief. Modern devices are MRI-compatible and rechargeable, with battery life exceeding 10 years. Dr. Bandikatla holds a Fellowship in Neuromodulation and Advanced Pain (London).
IBAP Clinics is Hyderabad's only dedicated multidisciplinary interventional pain clinic led by a UK-trained, dual-fellowship specialist — Dr. Vijay Bhaskar Bandikatla (FRCA, FFPMRCA, CCT UK, Fellowship Neuromodulation London). Every procedure is performed under live fluoroscopic or ultrasound guidance. We offer the full spectrum from diagnostic nerve blocks and intradiscal procedures to neuromodulation implants — under one roof. We also provide unbiased second opinions for patients who have been advised surgery. Main clinic: Banjara Hills. Branch: Madeenaguda. Senior Consultant, Apollo Hospitals.